Contents Home Performance IV Therapy: Benefits, Safety, and What to...
Read More

Reviewer | 22nd April | Read time – 11 mins
B12 is the largest and most structurally complex of all the vitamins, and the only one that contains a metal ion. It is also the one most likely to be silently deficient in the Indian population — not because people aren’t eating enough, but because the gut mechanisms required to absorb it are unreliable, decline with age, and fail entirely in a significant minority of people. By some estimates, more than two-thirds of Indian urban men have low B12 status. For vegetarians and vegans, the figure is higher still.
The consequences of B12 deficiency don’t announce themselves clearly. Fatigue is the most common complaint, but it is diffuse and easily attributed to other causes. Neurological symptoms — tingling in the hands and feet, memory lapses, low mood, slowed thinking — develop gradually and are often dismissed as stress or ageing. By the time a standard blood test shows deficiency, depletion has usually been building for months or years. And some of the neurological damage, if left long enough, is irreversible.
This article covers what B12 IV therapy does and where the evidence is strongest, how B12 functions in the body, why IV delivery matters when oral supplementation is unreliable, who is most at risk and who should not receive IV B12, what a session involves, what it costs in India, and what to look for in a provider.
B12 IV therapy is not a general wellness top-up. It is a targeted intervention for a specific and common deficiency — one with documented consequences across neurological, haematological, and cardiovascular systems. Here is what the evidence says for each benefit area.
B12 is a cofactor for methylmalonyl-CoA mutase, an enzyme essential to mitochondrial energy metabolism. When B12 is insufficient, this pathway slows — cells produce less ATP, and the result is fatigue that doesn’t respond to sleep or lifestyle changes because the problem is metabolic, not behavioural. A 2024 expert consensus review confirmed that B12 deficiency can cause variable symptoms including profound fatigue, and that timely correction is essential to prevent irreversible complications. [1]
The nuance worth understanding: a 2021 systematic review and meta-analysis of 16 RCTs found that B12 supplementation did not significantly improve cognitive function or fatigue in people without overt deficiency or advanced neurological disorders. [3] The implication is direct — B12 IV therapy works best when deficiency is present and is driving the symptom. It is not a stimulant. It is a correction. Patients with documented low B12 status, or with the risk factors that predict deficiency, are the right candidates.
This is where the stakes are highest. B12 is required for the synthesis of myelin — the fatty sheath that insulates nerve fibres and allows electrical signals to travel efficiently. Without adequate B12, myelin degrades. The neurological consequences include peripheral neuropathy, cognitive slowing, mood disturbances, and in severe or prolonged cases, irreversible spinal cord degeneration. A 2025 systematic review of RCTs confirmed that B12 deficiency causes peripheral neuropathy, cognitive impairment, and myelopathy, and that supplementation produces measurable neurological improvements in deficient patients. [2]
For early or moderate deficiency, the neurological effects are largely reversible with treatment. For long-standing severe deficiency, partial recovery is typical. Higher B12 status from mid- to late life is associated with slower rates of cognitive decline, with B12 supporting brain neurotrophic factors that maintain the structural integrity of myelin and glial cells. [4] IV delivery is particularly relevant for patients with absorption issues — because the gut limitation that caused the deficiency will also limit oral treatment.
B12 is required for the conversion of homocysteine to methionine, which feeds into the methylation cycle that produces SAM-e — the body’s primary methyl donor and a key substrate for serotonin, dopamine, and noradrenaline synthesis. When B12 is depleted, this pathway slows, neurotransmitter production falls, and mood deteriorates. The same 2021 meta-analysis found no significant effect of B12 supplementation on depressive symptoms in people without overt deficiency [3] — reinforcing the point that this therapy corrects deficiency, it doesn’t enhance already-normal function.
B12 deficiency raises homocysteine — an amino acid that, at elevated concentrations, damages arterial endothelium, promotes atherosclerosis, and increases risk of heart disease and stroke. Elevated homocysteine is considered an independent cardiovascular risk factor, and B12 deficiency-induced hyperhomocysteinemia is particularly prevalent in vegetarians, with mean homocysteine above 10 µmol/L reported in the majority of vegetarian studies. [8]
India is a particularly important context here. A study of middle-aged Indian men found that 67% had low B12 concentration and 58% had hyperhomocysteinemia — with urban middle-class participants showing the highest rates at 81% and 79% respectively. Vegetarians had 4.4 times higher risk of low B12 than non-vegetarians. [6] B12 IV therapy normalises B12 status rapidly, reducing homocysteine and addressing one of the most modifiable cardiovascular risk factors in this population.
B12 is required alongside folate for DNA synthesis in rapidly dividing cells — including the red blood cell precursors in bone marrow. Deficiency causes megaloblastic anaemia: red blood cells that are abnormally large, structurally fragile, and unable to carry oxygen efficiently. Early recognition of haematological manifestations is essential to prevent irreversible complications, and in cases of B12 malabsorption, oral supplementation is likely insufficient — parenteral administration is recommended. [10] IV or intramuscular delivery ensures the repletion reaches the bloodstream regardless of gut absorption status.
Reviewer | Date | Read time
B12 exists in several forms — cyanocobalamin, hydroxocobalamin, methylcobalamin, and adenosylcobalamin. The two that matter biologically are methylcobalamin and adenosylcobalamin: the active forms that serve as cofactors in the body’s two key B12-dependent reactions. Methylcobalamin supports the methionine synthase reaction — converting homocysteine to methionine and feeding the methylation cycle. Adenosylcobalamin supports the methylmalonyl-CoA mutase reaction in the mitochondria, driving energy metabolism and odd-chain fatty acid processing.
Hydroxocobalamin is the form most commonly used in IV therapy. It is stable in solution, has a longer half-life than cyanocobalamin, and is converted to both active forms in the body. It also has a secondary clinical use: hydroxocobalamin binds cyanide and is used as an antidote in cyanide poisoning. In therapeutic B12 doses, this property is irrelevant, but it speaks to the molecule’s binding affinity and retention in tissues.
The absorption story is what makes IV delivery relevant. Dietary B12 requires intrinsic factor — a glycoprotein secreted by parietal cells in the stomach — to be absorbed in the terminal ileum. When intrinsic factor-driven absorption fails, deficiency progresses regardless of dietary intake, and clinical consequences can appear within two to five years. [5] Intrinsic factor declines with age, is absent in pernicious anaemia, and is disrupted by atrophic gastritis, H. pylori infection, metformin use, and proton pump inhibitor therapy. IV delivery bypasses the entire intrinsic factor pathway.
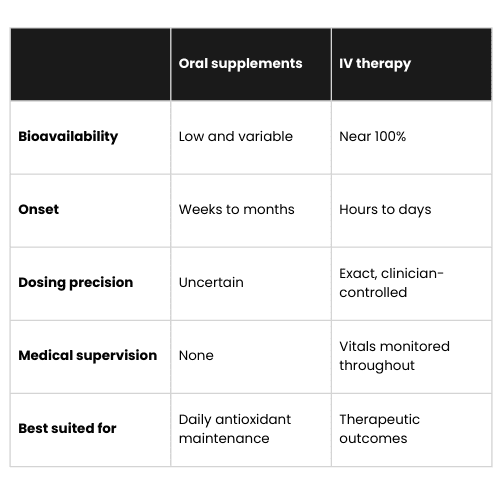
For patients without absorption issues and with mild deficiency, high-dose oral B12 can work through passive diffusion — a small percentage of a very large oral dose crosses the intestinal wall without intrinsic factor. This is why oral B12 at 1000–2000µg daily can eventually correct deficiency in some patients.
The problem is speed, reliability, and ceiling. A 2024 systematic review and meta-analysis found that sublingual and oral B12 achieved comparable serum levels to intramuscular injection over time in patients with non-malabsorptive deficiency — but the key phrase is ‘over time’. [9] For patients with neurological symptoms, megaloblastic anaemia, or documented malabsorption, waiting weeks for oral therapy to gradually raise levels is a clinical risk. IV or intramuscular delivery achieves repletion within the session and begins driving cellular repair immediately.
The other consideration is the absorption barrier itself. In patients with B12 malabsorption — pernicious anaemia, post-gastrectomy, inflammatory bowel disease, or severe atrophic gastritis — oral supplementation is likely insufficient and parenteral administration is recommended as the appropriate route. [10] For these patients, IV is not a preference — it is the clinical standard.
If you want to know whether B12 IV Therapy fits what you’re experiencing, our clinical team is happy to walk you through it
The safety profile of B12 IV therapy is excellent. B12 is water-soluble and any excess is renally excreted — there is no accumulation toxicity at therapeutic doses. Serious adverse reactions are rare and typically relate to the excipients in the preparation rather than B12 itself.
The most common reaction is a transient flushing sensation or a mild warmth at the injection site. Hydroxocobalamin can impart a reddish or orange tint to the urine and, temporarily, to the skin — this is harmless and resolves within hours. Very rarely, patients with a history of cobalt or B12 hypersensitivity may experience a reaction; screening for this in the clinical consultation covers it.
One contraindication worth noting: Leber’s hereditary optic neuropathy — a rare mitochondrial genetic condition — is a contraindication for hydroxocobalamin, which can accelerate optic nerve degeneration in affected individuals. This is uncommon but should be screened in patients with a family history of unexplained vision loss. Cyanocobalamin is also contraindicated in patients with known cyanide metabolism disorders. In standard wellness and deficiency-correction contexts, neither of these is a common issue.
In India, as with all IV therapy, the relevant question is preparation quality. Pharmaceutical-grade hydroxocobalamin from a licensed pharmacy, administered through sterile single-use equipment, is the baseline. Ask the clinic directly about their sourcing and oversight.
Real contraindications exist and require direct screening. Severe kidney disease is the most important: magnesium and calcium are renally cleared, and impaired kidneys cannot handle therapeutic IV doses. Hyperkalaemia, severe cardiac arrhythmias, and haemochromatosis (IV vitamin C enhances iron absorption) are also contraindications. Patients on digoxin need careful calcium monitoring — the two interact. Anyone with heart failure or fluid-sensitive conditions needs physician clearance before any IV therapy.
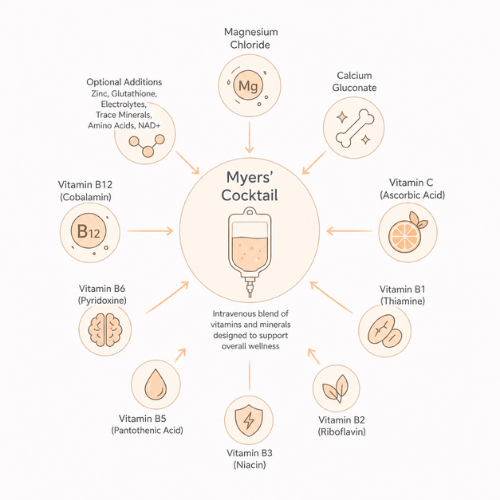
Hypocalcaemia is a theoretical risk with magnesium-heavy formulations — the two minerals compete for cellular entry. A well-formulated Myers’ Cocktail includes calcium precisely to buffer this. Clinics substituting components without understanding the rationale introduce risks that the original formula was designed to avoid.
In India, the same question applies here as with any IV therapy: where does the preparation come from? Pharmaceutical-grade ingredients, prepared in a licensed pharmacy under sterile conditions, are non-negotiable. Improvised formulations in unmonitored spaces are a different and significantly riskier proposition. Ask directly. The answers — and any hesitation in giving them — are informative.
The consultation covers your health history, symptoms, any medications, and relevant risk factors — pernicious anaemia, metformin use, vegan or vegetarian diet, age over 50, or a history of gut conditions. If you haven’t had recent B12 bloodwork, many clinics will recommend a baseline before proceeding, particularly if the goal is deficiency correction rather than maintenance.
The infusion is brief. B12 at typical wellness doses (1000–5000µg in a small volume of saline) runs 15 to 30 minutes. The cannula goes into the forearm in the usual way. Most patients feel nothing during the infusion. The reddish-orange colour of the hydroxocobalamin solution is striking — it often prompts questions — but it’s simply the natural colour of the molecule and not a cause for concern.
Leaving the clinic, improvement timelines depend on the degree of deficiency. For patients with significant depletion, energy improvements often become perceptible within 24 to 72 hours as B12 begins restoring metabolic and neurological function. Neurological symptoms — tingling, numbness, cognitive fog — typically improve more gradually over weeks of treatment, with more severe or long-standing symptoms taking longer. Mood improvements are often reported within 1 to 2 weeks. There is no recovery period and no activity restriction.
B12 IV sessions are among the more affordable IV nutrient protocols, typically ranging from ₹1,500 to ₹4,000 in Indian metro cities. The range reflects preparation grade, clinical infrastructure, and whether a consultation and monitoring are included.
For active deficiency correction, an initial course of weekly or bi-weekly sessions over 4 to 6 weeks is often appropriate before moving to monthly maintenance. For patients with ongoing malabsorption, regular sessions are the long-term standard. True Drip’s pricing is listed transparently at truedrip.in.
A fair price covers pharmaceutical-grade components from a licensed pharmacy, a clinical consultation, trained administration, monitoring during infusion, and access to a physician if something unexpected occurs. When a number looks unusually low, something in that list has been removed. True Drip’s pricing is listed transparently at truedrip.in. Most patients who come for energy or recovery goals find that a course of two to three sessions over a month produces more sustained results than a single infusion.
If you want to know whether B12 IV Therapy fits what you’re experiencing, our clinical team is happy to walk you through it

The case for B12 IV therapy in Hyderabad is more direct than for almost any other protocol — because the local population is among the most B12-deficient in the world. Subnormal B12 status is prevalent in 50–70% of vegetarians and vegans in India [7], and Hyderabad’s demographics reflect this. The city has a large vegetarian population, a significant proportion of whom have never been screened for B12 status and have been subclinically depleted for years.
The tech and professional workforce adds another layer. Metformin — widely prescribed for type 2 diabetes and insulin resistance, both common in the city’s working population — depletes B12 through gut absorption interference. Proton pump inhibitors, also commonly prescribed, reduce gastric acid and impair B12 release from food. Many patients in Hitech City, Gachibowli, and Madhapur are on one or both of these without any B12 monitoring.
True Drip’s clinical team screens for deficiency risk factors as standard before any B12 session. For patients who want to know their actual B12 and homocysteine status before beginning, we can advise on appropriate testing. Every session uses pharmaceutical-grade hydroxocobalamin, administered under clinician supervision with continuous monitoring.
Every session at True Drip includes a pre-infusion consultation, pharmaceutical-grade formulation, and clinician-supervised delivery. The specific Myers’ formula can be adjusted for your presentation — that’s the point of clinical oversight rather than a fixed retail protocol.

The direct intravenous delivery of hydroxocobalamin — the active form of vitamin B12 — in a small saline solution. It bypasses the gut absorption pathway entirely, making it effective for patients with malabsorption as well as those seeking faster repletion than oral supplementation provides.
Vegetarians and vegans, people over 50, anyone on metformin or long-term proton pump inhibitors, patients with pernicious anaemia or inflammatory bowel disease, anyone with unexplained fatigue or neurological symptoms, and anyone with confirmed low B12 on bloodwork. It is also used for maintenance in patients whose absorption issues make ongoing oral supplementation unreliable.
Energy and mood improvements are often perceptible within 24 to 72 hours of the first session for patients with significant deficiency. Neurological symptoms — tingling, numbness, cognitive fog — improve more gradually, typically over weeks of regular treatment. The more severe or long-standing the deficiency, the longer full recovery takes.
IV and intramuscular delivery are both parenteral routes that bypass gut absorption — the key advantage over oral. IV delivery distributes slightly faster. For patients with malabsorption, both are significantly more effective than oral. For patients without absorption issues and with mild deficiency, high-dose oral B12 can work, but is slower.
Hydroxocobalamin is the standard for IV and intramuscular therapy — it is stable, has a long tissue half-life, and is converted to both active forms (methylcobalamin and adenosylcobalamin) in the body. Methylcobalamin is sometimes preferred for neurological presentations specifically, as it directly supports the methionine synthase pathway.
Serious side effects are rare. Mild flushing or warmth may occur. Hydroxocobalamin gives urine and occasionally skin a temporary reddish-orange tint — this is harmless and resolves within hours. Patients with cobalt or B12 hypersensitivity should inform their clinician before proceeding.
Patients with Leber’s hereditary optic neuropathy should not receive hydroxocobalamin. Those with cyanide metabolism disorders should not receive cyanocobalamin. Both are rare. Anyone with a known allergy to cobalamin or its excipients should discuss alternatives with their clinician.
For active deficiency correction, weekly or bi-weekly sessions for 4 to 6 weeks, then monthly maintenance. For patients with ongoing malabsorption conditions, regular monthly sessions are the clinical standard. For maintenance without deficiency, quarterly sessions are typically sufficient.
Yes, and it’s worth doing. Serum B12, homocysteine, and methylmalonic acid are the most informative markers. Standard serum B12 alone can miss functional deficiency — homocysteine and MMA are more sensitive indicators. True Drip’s clinical team can advise on what testing makes sense for your situation.
Studies of Indian urban populations show that up to 67–81% of men have low B12 concentrations, with vegetarians at significantly higher risk. [6] India’s predominantly vegetarian diet, combined with low awareness of B12 monitoring and limited screening in routine health checks, makes silent B12 deficiency one of the most prevalent and underdiagnosed nutrient conditions in the country.
If you want to know whether B12 IV Therapy fits what you’re experiencing, our clinical team is happy to walk you through it
Contents Home Performance IV Therapy: Benefits, Safety, and What to...
Read MoreContents Home Hydration IV Therapy: Benefits, Safety, and What to...
Read MoreContents Home Immunity IV Therapy: Benefits, Safety, and What to...
Read MoreContents Home Magnesium IV Therapy: Benefits, Safety, and What to...
Read More